Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/load.php on line 651
Notice: Trying to access array offset on value of type bool in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/theme.php on line 2241
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387 Reinventing Medicaid – RI Future Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
After the successes of Governor Gina Raimondo’s Reinventing Medicaid task force, today, at the Kent County YMCA, she announced a new initiative to overhaul the state’s healthcare system as a whole. Titled the Working Group for Healthcare Innovation, the group, under the leadership of Elizabeth Roberts, the Secretary of Health and Human Services, seeks to improve Rhode Island’s healthcare landscape, making it more competitive with other New England states.
Gov. Raimondo and Sen. Whitehouse with YMCA campers after signing the healthcare reform executive order
“Today we are talking about keeping a dialogue going that you so successfully started on earlier this year,” Raimondo said, referring to Reinventing Medicaid. She added that she seeks to take the work that was done there, in the public healthcare system, and move it forward.
“Today is about bringing that same level of innovation in all that we do in healthcare delivery in the state of Rhode Island,” she said.
The Governor has set forth four specific goals for the task force to achieve, under specific deadlines. They are to develop a global healthcare spending cap; plan out and implement the “80 by ’18,” goal, which would tie 80 percent of healthcare payments to quality by 2018; bring the state’s healthcare system technologically up to date; and establish a framework to achieve health and wellness goals outlined by the Centers for Disease Control.
Raimondo said that the biggest goal, which all of these are to work together to achieve, is to reduce the costs of healthcare, improve outputs, and improve the patient experience. She said that these goals are the “holy grail,” of providing healthcare, and making Rhode Island more effective overall.
“I believe it’s doable, I know it’s doable. It’s doable if we commit ourselves,” she said. “We’ve got to catch up and we’ve got to be competitive. Rhode Island has to be competitive.”
The focus of the task force will draw from suggestions made by a group of healthcare stakeholders that Governor Raimondo received back in December. Many members of this group, which was put together by United States Senator Sheldon Whitehouse and Rhode Island Foundation President Neil Steinberg, will now be serving with on the new task force.
Whitehouse also spoke in support of Raimondo’s initiative, citing that the United States spends more money per capita in relation to life expectancy than almost every other developed country. The United States’ life expectancy is also lower than many countries that pay less per capita. Whitehouse also mentioned that since 1960, health care expenditures have risen from $27.4 billion to $2.8 trillion. Healthcare spending has declined in recent years, but reducing costs remains a priority.
“It’s not a system where you can tell it what to do and it’s going to change,” Whitehouse said, speaking about how healthcare reform works. “You actually need to change the system. What you say is a whisper, how you pay is a shout.”
Secretary Roberts, who will head the group, said that even though healthcare reform is a very complex issue, the working group can find a solution because they want to get the community involved in the process. Rather than just having a conversation about what needs to be done, Roberts said, there will be collaboration on both ends of the project. By doing this, they will create a long-term plan.
“I am excited to see the Governor take a very direct interest, and give us a very direct charge, because that, to me, is absolutely crucial to a statewide approach,” Roberts said about her enthusiasm to begin working. “I am excited to see the range of people who have stepped forward to participate, and know that we will make some real progress.”
Roberts has had experience working with the Rhode Island healthcare industry in the past, as former Lieutenant Governor during the Chafee Administration. Roberts has also worked in health insurance before she was involved in government, and as a legislator, she chaired the Health Committee.
“Many of us have met before, and have worked together before,” she said. “But the charge of the Governor, to really come together, and really make some measurable differences, is going to move us forward.”
The Working Group for Healthcare Innovation will begin meeting in August, and give its first set of recommendations to Governor Raimondo in December. Members of the group come from several communities, including government, insurance, hospital workers, labor, and business. There are 36 total members.
SEIU 1199, representing about 4,000 health care workers in RI, held a press conference to announce a series of initiatives “to improve the way the state invests in Medicaid-funded programs in long-term care and create a pathway to living wages for caregivers.”
The press conference was part of a “Day of Action” at the State House, and was followed by SEIU members presenting their ideas to their state reps and senators ahead of the day’s legislative session.
“I love my residents like my own family, but at the end of the day, I don’t bring home enough money to take care of my two daughters,” said Nichole Ward, a certified nursing assistant (CNA) at Greenville Skilled Nursing and Rehab in Greenville, who spoke of the difficulty of not earning a living wage. “After working hard, being on our feet, taking care of people for 40 hours a week, I shouldn’t have to choose between my electric bill and school supplies for my kids. We deserve at least $15 an hour.”
Patrick Quinn, executive director of SEIU 1199 and a member of the Reinventing Medicaid working group, outlined the eight points of SEIU’s plan to both cut Medicaid costs and increase wages for frontline medical workers while improving health outcomes. The eight points are expanded upon in a white paper entitled From the Frontlines to the Bottom Line.
1. Create a value based purchasing program to improve care quality and staffing in nursing homes and reduce re-hospitalization.
2. Increase transparency of “related party” finances and reporting, in effort to reduce waste, fraud, and abuse.
3. Target any nursing home rate reductions toward costs unrelated to the provision of direct care, such as Fair Rental Value and “home office” charges.
4. Focus increased revenue and rate restoration initiatives on direct resident care and workforce stability.
5. Claw Back: Recoup Medicaid reimbursements that are not used for their intended purpose, especially in regards to direct labor.
6. Cap Medicaid reimbursement for executive compensation based on facility size.
7. Realize Medicaid savings though more energy efficiency initiatives.
8. Expand Rhode Island’s Paid Family Leave Program from 4 to 6 Weeks.
Speaking in support of the SEIU’s effort was Jenn Steinfeld of the Women’s Fund of Rhode Island, who sees this as both a social justice and gender equity issue.
It’s a gender issue on two fronts, says Steinfeld, because women live longer, and therefore make up 74 percent of the elderly patients in the Medicaid system and women make up 90 percent of the direct care workforce. Additionally, the over representation of minorities in the field makes this a racial justice issue, notes Steinfeld.
CNAs Dawn Auclair and Manoucheka Robert both spoke about the attachment they have to their patients, the importance of their work, and their difficulty in performing this valuable work for such low pay.
Sarah Nolan, who works for the SEIU International Policy Department in Washington DC, said that the white paper they have released focuses on both short and long term solutions to the problems in Medicaid quality and cost. She also stressed the importance of front line medical workers playing a role in these discussions.
Near the end of the press conference, CNA Nichole Ward explained that experience is key when dealing with patients. Cutting costs and worker turnover can raise the stress level of front line health care workers, and residents in nursing homes can sense that stress, even if healthcare workers think they are hiding it.
Such an environment cuts against the efforts to improve health care.
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
The 7th Annual Budget Policy Conference, a fundraiser for the Economic Progress Institute (EPI), had a timely theme: “Medicaid on the Move.”
Since Governor Gina Raimondo announced a Medicaid crisis in February and the creation of a working group of “27 members from across health care, business, state government and community and nonprofit organizations” to deal with the crisis, the idea of “Reinventing Medicaid” has become a central part of the state’s 2016 budget process.
Medicaid is a state and federally supported system of health care that targets the most vulnerable and least represented people in our community, i.e. children, low income adults, the elderly and those with mental or physical handicaps. So special attention must be paid to the process of “reinventing” the system and therefore an appropriate target for a progressive economic institute such as EPI to address.
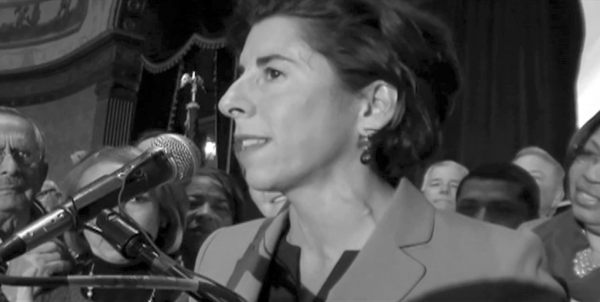
Governor Raimondo gave the opening address to the breakfast crowd, mostly made up of medical policy wonks and EPI supporters. She used the opportunity to press for a $10.10 minimum wage and for an increase in the earned income tax credit from 10 to 15 percent, possibly her two most progressive ideas in her 2016 budget proposal.
Moving onto Medicaid, Raimondo insisted that her goal in pulling together the working group is “not about kicking people off Medicaid” but “getting people cared for in the lowest cost environment.”
Raimondo acknowledged that the EPI and many of those in the audience are more concerned with social justice and economic justice than they are with short term budget fixes when she said, near the end of her speech, “Your stubborn idealism is a good thing for Rhode Island, so don’t lose it.”
Linda Katz, policy director and co-founder of the EPI, spent 14 minutes introducing the audience to the basic facts about Medicaid. In the video below I’ve combined the slides from her presentation with the talk she gave.
Katz is a member of the Reinventing Medicaid working group. The first weeks of work by the working group, Katz suggested, was preliminary. Now, as the working group prepares to move ahead and plan the implementation of the ideas presented, Katz says that she’s “looking forward to part two, where we take a deeper dive into Medicaid.”
Cindy Mann, former Medicaid Director in the Obama Administration, began her talk noting that this July will mark the 50th anniversary of Medicaid. Medicaid, says Mann, “is constantly reinventing itself.”
Over the course of her talk Mann explained exactly who Medicaid serves, and why Rhode Island is in many ways both an outlier and a leader in the way we administer the program. In the video below I’ve combined the slides from her presentation with the talk she gave.
For instance, “Rhode Island has, as a population, more elderly and disabled” than many other states, said Mann. Three percent of our Medicaid enrollees account for 70 percent of our Medicaid spending.
Mann made a special point to mention the medical care of the incarcerated, surely the population our society seems least vested in. When people in our prisons require outpatient care, that is, medical services the prison hospital is unable to meet, Medicaid covers the expense. Mann maintained that the state should make sure that “no one leaves jail without being assessed for health care coverage.”
Former Lt. Governor Elizabeth Roberts, who Governor Lincoln Chafee tasked with setting up the state’s health care exchange and who Raimondo put in charge of the working group, spoke last.
Roberts said that she and the working group instead worked to reform the system. “We did not remove benefits,” said Roberts. In addition to the recommendations of the working group, Roberts feels that there needs to be a pay increase for certified nursing assistants and home health care workers, who are being squeezed economically.
Roberts also agreed with Katz about the second phase of the working group’s mission. The “next 2 months,” said Roberts, “will be more important than the last 2.” The working group issues its final report in July.
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
The Reinventing Medicaid working group unveiled 55 initiatives that are projected to result in $85.5 million in savings. Former Lt. Governor Elizabeth Roberts, tasked by Governor Gina Raimondo to head up the group, said that they are still working through over 200 suggestions, some of which may be included in the final report.
“A deadline induced series of last minute proposals,” said Roberts, “will be considered over the next week.”
This was the 3rd Reinventing Medicaid working group meeting and it was held in the fourth floor boardroom of CCRI in Warwick ahead of the working group’s April 30 report of proposed 2016 RI state budget initiatives. The working group’s final report is due in July, but working group co-chair Dennis Keefe, of Care New England, cautioned that “You can’t do reform in a year. It takes five, six, seven years…”
Today’s meeting took the form of a two and a half hour “facilitated discussion” with a PowerPoint presentation and specialized iPads that allowed working group members to type their questions, concerns and ideas onto the screen. This procedure had the benefit/drawback of anonymizing feedback from working group members, so it was hard to tell, for instance, who was worried about capping hospital executive salaries and who was worried about EBT card abuse.
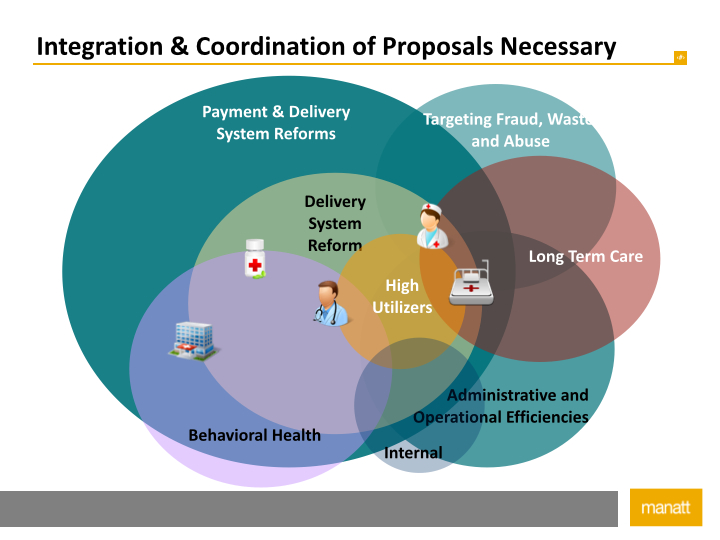
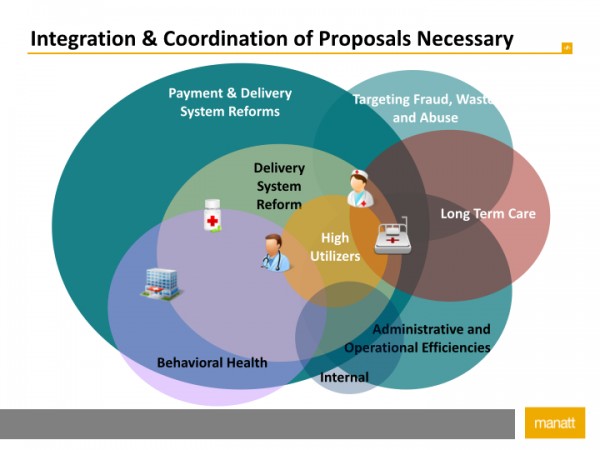
The 55 initiatives were group by theme:
Payment and Delivery System Reforms: initiatives related to transforming Rhode Island Medicaid into one which pays for quality and value, rather than volume, and which promotes quality of care and patient experience.
Targeting Fraud, Waste, and Abuse: initiatives related to ensuring that Medicaid programs operate in compliance with state and federal law and regulation, and rooting out wasteful, unnecessary, or fraudulent spending and utilization.
Administrative and Operational Efficiencies: initiatives related to streamlining and improving state oversight of the Medicaid program.
A total savings of $85.5 million is projected so far:
Some initiatives were discussed singularly, others were grouped, and more than half were not discussed at all. The first idea to be presented was a plan to “implement an incentive program to reduce unnecessary hospital utilization funded by a 5% decrease in hospital payment rates.” This is projected to save the state $15.7 million. According to the working group:
This initiative would eliminate the FY2016 rate increase for hospital services and reduce hospital rates by a further 5 % across both fee for service and managed care. Achievement of savings in the managed care products (Rite Care, Rhody Health Partners and Rhody Health Options) will be accomplished through modifications to the capitation rate.
The $31 million saved would be re?invested in a hospital incentive program. Hospitals would have the opportunity to earn back a portion of the $31 million based on achieving performance goals around reduction of unnecessary utilization, reduction of avoidable re-admissions, and improved coordination of care. The incentive payments earned would be paid in September 2016.
What this means is that the 5 percent in “savings” would be placed into a “pool” which hospitals can claim the following year, based on the hospitals ability to satisfy certain metrics. Medicaid dollars would be unavailable for re-hospitalizations, hospital borne illnesses and the like. Instead, the hospitals will be able to claim these dollars only if they can show that they have attained certain patient health metrics. Such a scheme may require “fast statutory changes” from the General Assembly.
The next initiative would “implement an incentive program to reduce long stays in nursing homes, funded by a 3% decrease in nursing home payment rates.”
This initiative, which would impact both fee-for-service and managed care services, involves two components: a 3.0% reduction in rates and the elimination of an inflation related rate increase. Approximately half of the savings are associated with Rhody Health Options, and will be achieved through a reduction in capitation rates.
The $17.9 million saved would be re-invested in a nursing home incentive program designed to avoid long stays. The program would measure discharges to the community and re-hospitalizations, and offer incentive payments to facilities that achieve high ratings on both scores.
This initiative can be thought of as similar to the first initiative, except that it would apply to nursing homes instead of hospitals, with a similar emphasis on positive patient outcomes. This initiative is seen as important since nursing home care is one of Medicaid’s biggest expenses. Ultimately, nursing homes would be able to claim 2016 money in 2017 for moving patients out of nursing homes.
Savings of $4 million are projected through “home stabilization initiatives for target populations.”
The purpose of the state’s Health Begins with a Home Initiative (HBHI) is to make an organized set of Medicaid-funded health and home?stabilization services available to members of certain sub-populations. This innovative home and health stabilization program targets Medicaid beneficiaries who have complex medical or behavioral health conditions and are either homeless or at risk for homelessness or transitioning from high?cost intensive care settings back into the community.
The HBHI focuses on the following Medicaid beneficiaries:
Target Group #1: Medicaid-eligible children and youth with behavioral health needs in the custody of the RI Department of Children, Youth, and Families (DCYF) who are at risk for or transitioning from institutionally based or residential treatment facilities, or congregate care; and the parent(s)/caretaker(s) of these children living in the community.
Target Group #2: Medicaid-eligible adults between the ages of 19 and 64 with serious behavioral health or physical conditions who are homeless or at risk of homelessness subsequent to military service, health treatment, or incarceration.
Target Group #3: Persons with disabilities, elders, and those who are transitioning from institutionally-based care who have a history of homelessness, would otherwise be homeless, if not for the nursing home stay or would benefit from service upon transition due to length of stay in the institution.
Medicaid will not pay for housing, but it can support programs to keep people from becoming homeless. This is one part of the plan that will require money upfront to see savings later. Keefe said that this is the kind of program where investment could be “significantly higher” for greater savings. He was very excited about this program.
The next idea was to “scale up community health teams.”
Community health teams (CHT) work as an extension of a primary care office to meet the social and behavioral needs of patients. They are a group of providers such as social workers, community health workers, nurse managers, and others who can directly address social, behavioral, and environmental factors affecting health and health behaviors. The CHT is modeled after similar highly successful programs in Vermont, Maine, North Carolina, and other states.
The RI Care Transformation Collaborative, an all-payer Medical Home initiative, is currently piloting two community health teams: one in South County and one in Pawtucket. Each community health team works collaboratively with CTC practices in that service area and health plans to identify high-risk patients. A number of other sites, including at least one Federally Qualified Health Center (FQHC), have developed their own Community Health Team with separate funding.
This initiative would quickly scale up the CHT and develop an organized, Medicaid-wide approach to CHT implementation. CHTs are provided lists of high-utilizer patients by the MCOs and collaborate with the Medical Home to address unmet needs. The result is improved utilization patterns, better health outcomes, and lower costs.
There is growing evidence, said the presenters, “that this model is effective.” Sally Finger, an adviser to the working group, said that costs are difficult to determine because the idea is so new. “This is really happening everywhere,” said Finger, “and it is not coordinated, which is why there isn’t much data on savings.”
The idea reminded me somewhat of former Rhode Island Department of Health Executive Director Michael Fine’s idea for Neighborhood Health Stations. Note also that we already service about a third of Rhode Island’s Medicaid recipients through nine community health centers represented by the Rhode Island Health Center Association. Community-based primary health care is definitely the right direction to go in.
The next two initiatives discussed were grouped together. Each would reap savings of about $1 million for the state.
Redesign CEDARR services program, transition to community health team approach
In keeping with the principles of paying for value in the Medicaid delivery system and reducing waste, this initiative will redesign the Comprehensive, Evaluation, Diagnosis, Assessment, Referral, Re-Evaluation (CEDARR) Family Center package. This redesign will include a discontinuation of the Family Care Plan Review, reduce the amount of Health Needs Coordination services, as well as transfer Direct Service Review functions of the CEDARR Family Centers to state staff.
Move out-of-plan services for children with special healthcare needs into managed care
In an effort to increase efficiency of care and coverage for high-?utilizing populations, this initiative will integrate services for children with special health care needs into the continuum of care of the Medicaid Managed Care Organizations (MCOs). Services that have been out of plan for this population and will now be integrated into the MCO scope include Home Based Therapeutic Services (HBTS), Personal Services and Supports (PASS), and Respite care. Through the integration of these and like services, this initiative will provide flexibility to the MCOs to provide more evidence-?based, clinically appropriate, lower-?cost services to children and adolescents.
The coordinating of these systems will, according to the working group, “optimize care” and “reduce costs.” But the question was raised, “Is the plan implementable and can the results of the plan be evaluated?” Open questions like this might call into question the estimates on savings.
The last of the big six ideas was to “coordinate care management for those with severe and persistent mental illness (SPMI).”
This initiative would create a population-?based health home approach for persons living with a serious mental illness. The program will reduce medical, pharmacy and behavioral health expenses for the population by better coordinating their care. All members will be attributed to an accountable health home. Providers will be paid a capitated rate for care coordination, and be incentivized for outcome measures and utilization.
In Rhode Island, there are currently 10,450 people who would be affected by this plan. Many of the pieces of this plan are already in place. It is thought that the state will save $3 million.
The next phase of the discussion concentrated on six initiatives targeting waste, fraud and abuse. This would included Electronic Visit Verification (EVV) for home health care workers (perhaps through a smart phone app) to ensure that the state “does not pay for services which are not actually delivered.” Savings could also be found by enrolling patients into Medicare, if eligible. Predictive modeling computer systems would “examine provider reimbursement policies” as well as search for inconsistencies and errors in payments.
The working group also believes that “enhanced residency verifications” that is, making sure that Rhode Island only pays for the Medicaid of Rhode Islanders, may save some money, though it was admitted that residency is “more complicated than it seems.” The determination of residency rests on the intent of the patient, which is a difficult to dispute federal standard.
Next a suite of 13 ideas to reform long term care were quickly examined. The working group did not delve too deeply into the specifics, but it was noted that the state may be spending too much on Hospice care.
Towards the end of the presentation Jim McNulty, a mental health advocate, said that “I like a lot of what I see here,” but added that “implementation of all these ideas will be extremely difficult.”
The April 30 report will be much more comprehensive. We should expect to see more ideas put forward and for Governor Raimondo’s goal of $90 million in cuts to be made. The General Assembly then goes to work dissecting the working group’s plan as part of its arduous budget process.
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Since two-thirds of minimum wage earners are women, Governor Gina Raimondo says that raising the minimum wage to $10.10 is an important way to help women and their families in Rhode Island. But Nicholas Oliver, executive director of Rhode Island Partnership for Home Care, Inc., a group that advocates for the home health care industry here in Rhode Island, says that the governor is “being a bit disingenuous, and we’ve seen that her messaging is a bit inconsistent.” More than 88 percent of home health care workers are women, and Raimondo’s budget isn’t helping them.
The governor is “saying that she wants to be an advocate for home care,” continues Oliver in a phone conversation, “particularly with this working group Reinventing Medicaid, but frankly we haven’t seen her put her money where her mouth is. She put into her budget proposal last month a freeze on home health care for another consecutive fiscal year.”
In testimony before the Senate Labor Committee hearing on the $10.10 minimum wage, Oliver explained that “Medicaid home and community based service rates have been frozen for the past seven consecutive fiscal years. However, much of that last rate increase in 2008 was rescinded the following fiscal year due to state budget constraints. So what we’re really talking about is 13 years since a rate increase…”
Medicaid reimbursements for home health care services are $17.68 an hour in Rhode Island. In addition to the worker’s salary, that money has to cover insurance, licensing, utilities, compliance and other expenses. “Many of our direct care staff, CNAs and home makers are earning wages at or slightly above the minimum wage. At current reimbursement rates we cannot afford to provide them a wage that is adequate, let alone competitive to their counterparts in nursing homes and hospitals that have received increases by the General Assembly almost every year.”
Medicaid reimbursements for similar services in Connecticut and Massachusetts are $24.40 and $24.64. “Why would someone work for minimum wage in a position that requires licensing by the Department of Health, continuing education to maintain that licensure, perform services that include toileting, bathing and feeding patients, at the same wage as someone working in retail or hospitality?” Oliver asked the Senate Committee, “The job market is responding with a resounding ‘no’ as many provider industries are having trouble hiring and maintaining direct care staff to fill the growing need for these services by Medicaid beneficiaries.”
The problem in finding workers for the money available is especially acute outside Providence, in places like southern Rhode Island and Woonsocket. Many workers are simply crossing the border into neighboring states where the money is better.
“We don’t want to oppose increasing the minimum wage,” says Oliver, “We’re really disappointed that the governor is proposing to increase the minimum wage and wants to be an advocate for minorities and women and single parents, but at the same time her message is inconsistent when it comes to health care because she’s saying, ‘Let’s increase wages for these folks, but not you, even though you’re a representative of the same work force I try to advocate for.’”
In her 2016 budget proposal, Governor Raimondo has suggested a 3 percent cut to nursing homes and a 5 percent cut to hospitals. The Reinventing Medicaid working group will issue its report and suggestions for additional cuts later this month. You can view Oliver’s testimony before the Senate Labor Committee below:
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Imagine a plan sitting at the RI Department of Health (RIDOH) that would reduce health care spending in Rhode Island by 15 to 30 percent. A plan with the added benefit of improving health care outcomes “with a cutting edge technology that brings every Rhode Islander into world class care – as they need it, where they need it, when they need it, in a way that builds community instead of building profit for others.”
Neighborhood Health Stations are “basically community hospitals without walls,” says Dr. Fine in conversation with Richard Asinof of ConvergenceRI. Dr. Fine planned to build one station for every 12,000 Rhode Islanders, between 75 and 100 such stations in all. The first one was to be built in Central Falls.
Neighborhood Health Stations would locate pediatricians, internists, family physicians, dentists, nurse practitioners, licensed and registered nurses, advanced practice nurses, physician assistants, mental health and social workers, physical therapists and occupational therapists, pharmacists, emergency medical technicians and paramedics, registered dietitians, home health workers, promotoras, health coaches, navigators and other healthcare workers under one roof, in a facility that would also offer programs such as “nutrition courses, Zumba classes, or group counseling sessions.”
According to Dr. Fine, if we implemented this plan, we could shrink the hospital system in our state. “When you build out the full delivery system of one neighborhood health station for every community of 12,000 people,” says Dr. Fine, “it is very likely that we can reduce the total number of hospital beds by 40 to 45 percent. That means dropping [the number of hospital beds in Rhode Island] by about 900 beds.”
Governor Gina Raimondo’s budget proposes cutting $88 million from Medicaid’s $2.7 billion in spending, a 3 to 6 percent reduction. Since “Reinventing Medicaid” is being presented as an answer to an imminent disaster, improving the quality of health care or paying adequate wages to health care workers is taking a back seat to saving money.
That’s a shame, because a fully realized health care system of the kind imagined by Dr. Fine would attract business and investment to Rhode Island, while draconian cuts in services to our most vulnerable will have the opposite effect. If we could build Neighborhood Health Stations and make them work, “then health care spending becomes a business magnet. People come and locate businesses here, just because of our health care,” says Dr. Fine.
It’s a great idea, but not one that’s likely to happen. Since Dr. Fine’s departure, Neighborhood Health Stations seem in jeopardy. The new head of the RIDOH, Dr. Nicole Alexander-Scott, has yet to comment on the plan. But a more immediate reason for the plan’s quiet demise can be intuited.
“…if I have had one failure [while serving as director of the R.I. Department of Health],” said Dr. Fine, “if I want to be self-critical, [it’s] that I haven’t made it clear enough to people that we don’t have a problem with insurance, the problem is insurance. That thinking, that insurance, as a financial mechanism, can impact health, is a fundamental, categorical mistake.”
Dr. Fine saw his Neighborhood Health Stations as saving money by cutting out for profit insurance companies, and actually reducing the size of hospitals. The Reinventing Medicaid working group is comprised of a diverse group of people, but for-profit insurers and health-care providers have a prominent seat at the table. Timothy Babineau, MD, president and CEO of Lifespan, Peter Andruszkiewicz, president and CEO of Blue Cross Blue Shield of RI and Helena Foulkes, executive vice president of CVS Health and president of CVS/pharmacy will ensure that their corporate, for-profit interests are protected.
To Dr. Fine, Neighborhood Health Stations are the future of health care. “…if we don’t do it, all we’re doing is perpetuating a costly infrastructure that doesn’t work.” An infrastructure that will remain immeasurably profitable to those sitting at the top of certain health care empires.
The “artwork was created by Roger Williams University students, in consultation with students at Rhode Island College School of Nursing, to illustrate how Neighborhood Health Stations could enhance well-being in Rhode Island communities.”
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Two single-payer advocacy groups, Rhode Island Chapters of Physicians for a National Health Program (PNHP) and HealthCare-Now, have prepared a report that is highly critical of Governor Gina Raimondo’s Reinventing Medicaid initiative.
The PNHP/HCN-RI report identifies five areas of concern and concludes that “Governor Raimondo has made it impossible” to achieve the goal of developing “a plan to improve the quality of care Rhode Islanders receive and reduce the costs for Rhode Island taxpayers.” The areas of concern cited in the analysis are:
1. presenting faulty and misleading data and analyses
2. misidentifying “problems;”
3. requiring unjustified budget cuts within preselected “six major strategies’”
4. not permitting consideration of the actual problem: private health insurance companies generating enormous administrative costs and improperly rationing care
5. not permitting consideration of an effective solution: a comprehensive single payer health care program for all Rhode Island residents such as that proposed by H5387, a single-payer health care bill introduced by Representative Aaron Regunberg.
Governor Raimondo
The report says Raimondo overstates the percentage of the Rhode Island budget spent on Medicaid. She uses 31 percent, but the PNHP/HCN-RI report says the actual number is 22.1 percent. Further, Rhode Island’s expenditures are below the national average of 23.7 percent. And it should not be forgotten that most Medicaid expenses are reimbursed by the federal government dollar for dollar. Every dollar cut from state expenditures is two dollars cut from services.
The PNHP/HCN-RI report also accuses Raimondo of cherry picking data to paint the worst possible picture to create a false Medicaid crisis.
When Raimondo considers the drivers of high Medicaid costs, she ignores key problems. While Raimondo blames “High Utilization,” an “Aging Population” or “fraud, waste and abuse,” the PNHP/HCN-RI analysts note that her supporting data are questionable and we should be looking at the fact that “multiple payers create enormous excessive administrative costs and unfairly ration care.”
The report concludes by making the case for single-payer healthcare. Adopting such a program, says the PNHP, will:
Provide comprehensive health care coverage to all Rhode Island residents with most Rhode Islanders paying less for health care than they are currently paying;
Improve access to health care;
Save approximately $4000 per resident per year by 2024 and put more money into the Rhode Island economy.
Significantly reduce health care dollars spent on administrative costs and shift these dollars to actual provision of health care (providers would save almost $1 billion in administrative costs in the first year);
Decrease administrative burdens on health care providers and allow them to spend more time providing health care;
Eliminate the burden of health insurance costs and administrative obligations on Rhode Island businesses and thereby make them more competitive and profitable. In the first year, payroll contributions to the single payer plan would be over $1.2 billion less than current private health insurance premiums.
Contain health care costs (reduced administration and control over monopolistic pricing) would save 23% of current expenditures in the first year with larger savings in subsequent years.
Create a significant economic stimulus for the state by attracting businesses to and keeping businesses in Rhode Island because of reduced health insurance costs, a particular boon to small businesses and their employees.
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Near the end of the public commentary period of the Reinventing Medicaid Town Hall Meeting held in Providence, Bonnie Holder observed that, “The measure of a society is based on how we treat our most vulnerable… How did we ever get to the point where we accept it as a society where 1 percent of the population can have enormous wealth and the rest of us here are fighting?”
What the standing room only crowd of nearly 200 people gathered in the foyer of the Providence Community Health Center on Prairie Avenue were fighting for was the funds needed to provide care and sustenance for children, the elderly, the poor and the homeless. Governor Gina Raimondo is seeking to cut $90 million out of Medicaid, an item that takes up about a third of the budget. Because the federal government matches state medicaid spending, the total of lost dollars to medical services in our state could be nearly double that number.
A steady stream of commentators took the microphone to say that our medical system is already straining to meet the needs of our community. Wages are stagnant, demand is only going to grow, and the money needed to get the job done right is already too tight.
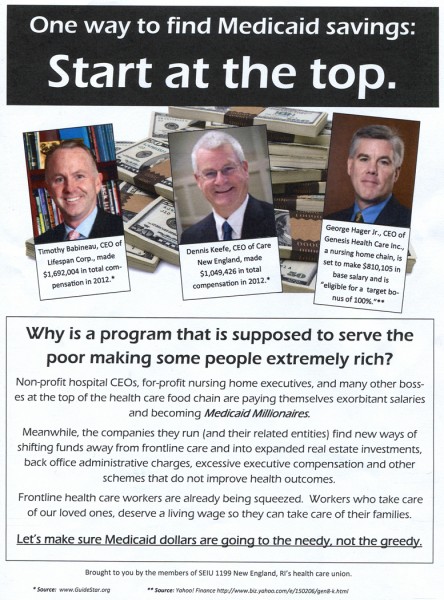
Undoubtedly there are savings to be had. Where those savings are to be found is a question of values and priorities. Are we going to force front line caregivers to work longer hours for less pay? Are we going to ask people to give up medical care and prescriptions that will enhance their quality of life? Or are we going to take a serious look at the salaries and compensation packages of some of the best paid CEOs in New England?
SEIU 1199 New England
The Town Hall in Providence was the second of four meetings. The first was held in Woonsocket on Monday night. The next one is scheduled for March 23 at the Peace Dale Library in Kingstown and the last one will be held on April 1 at the Portsmouth Fee Public Library in Portsmouth.
Stay tuned.
Former Congressman Ed Beard was the first speaker. Now a patient in a nursing home, Beard, now 74, suffers from Parkinson’s and was confined to a wheelchair. At one point a nurse’s assistant came forward to steady his hand so that he could hold the microphone. “I know cuts will be damaging,” he said, “Just be very cautious when you talk about the seniors. The seniors are a forgotten lot.”
“I am one of hundreds of CNAs in this state who provide personal, bedside care to elders in our nursing homes. My job is physically and emotionally demanding but highly gratifying… I am really concerned that the nursing homes are going to funding cuts again this year…”
“If we don’t have enough to help these people, to pay our nurses, what are we going to do? In our nursing homes, if we have 2 nurses for 6 patients now, what’s going to happen if we have a bunch of cuts?”
“It’s not pleasant to be poor. To wonder whether or not one will eat today, or have enough heat to heat one’s house or even to have a house to live in…”
“If my wife went to a nursing home, in three years I would be broke. I would have to go on welfare…”
“The corrections department is actually the largest provider of behavioral healthcare in the state…”
“These are people dependent on others for 24 hour care. They cannot safely remain at home, they’re aged and frail, they may have lost their independence, many of those closest to them have died, they rely on us for everything…”
“As a person living with mental illness and working in the mental health field, I want to stress the idea of peer support. Peer support is important to people living with mental illness… Medicaid should support peer supporters in the mental health system…”
“Permanent supportive housing is an inexpensive way to really effect some true Medicaid savings.”
“A ton of money is saved by being able to point them to either a health center or to a primary care doctor…”
“When we think about cutting some of the costs in Medicaid, home care only accounts for 5 percent of the money that is being spent…”
“Many executives make over six figures, and other executives make millions. Governor Raimondo has set an excellent example with taking a 5 percent pay cut to her salary. Perhaps our hospital and nursing home executives should do the same…”
“We have many patient cases where they cannot afford their medication, they stretch out their medication or split their pills or take their medication every other day. We then see that when these same patients become eligible for Medicaid, their compliance increases, and they become advocates in their own health care.”
“The nurses… throughout the state providing home healthcare, reimbursement rates have been frozen for eight years now…”
“I specifically want to talk about the significance of non emergency medical transportation…”
“Here’s what Medicaid pays for nursing home care: $6.30 an hour…”
“It’s just not what one does that matters, it’s how one does it. And how we choose to reform Medicare will have an impact for generations to come…”
“It’s established that the single greatest that reduces mortality among seniors is isolation…”
“More than 28,000 children in providence receive RICARE benefits…”
“I was distressed to hear about the Medicaid fund reductions. I know the federal government is making cuts…”
“I take care of children who, if there’s no nurse in the home, those parents don’t go to bed. And if there’s no nurse in the home for a couple of days, those parents cannot take care of that child…”
“If you have to increase what you provide in a healthcare setting and your dollars are being cut, there’s only a few places that money is going to come from. Labor and staff, food and medication. So if that’s what we’re looking at cutting, labor, food, staff and medication, shame on everybody in this state…”
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387


 SEIU 1199, representing about 4,000 health care workers in RI, held a press conference to announce a series of initiatives “to improve the way the state invests in Medicaid-funded programs in long-term care and create a pathway to living wages for caregivers.”
SEIU 1199, representing about 4,000 health care workers in RI, held a press conference to announce a series of initiatives “to improve the way the state invests in Medicaid-funded programs in long-term care and create a pathway to living wages for caregivers.” Speaking in support of the SEIU’s effort was Jenn Steinfeld of the Women’s Fund of Rhode Island, who sees this as both a social justice and gender equity issue.
Speaking in support of the SEIU’s effort was Jenn Steinfeld of the Women’s Fund of Rhode Island, who sees this as both a social justice and gender equity issue.
 The 7th Annual Budget Policy Conference, a fundraiser for the
The 7th Annual Budget Policy Conference, a fundraiser for the 

 In Rhode Island, there are currently 10,450 people who would be affected by this plan. Many of the pieces of this plan are already in place. It is thought that the state will save $3 million.
In Rhode Island, there are currently 10,450 people who would be affected by this plan. Many of the pieces of this plan are already in place. It is thought that the state will save $3 million.
 Since two-thirds of minimum wage earners are women, Governor Gina Raimondo says that
Since two-thirds of minimum wage earners are women, Governor Gina Raimondo says that 
 Imagine a plan sitting at the RI Department of Health (RIDOH) that would reduce health care spending in Rhode Island by 15 to 30 percent. A plan with the added benefit of improving health care outcomes “
Imagine a plan sitting at the RI Department of Health (RIDOH) that would reduce health care spending in Rhode Island by 15 to 30 percent. A plan with the added benefit of improving health care outcomes “ Neighborhood Health Stations would
Neighborhood Health Stations would