Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/load.php on line 651
Notice: Trying to access array offset on value of type bool in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/theme.php on line 2241
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387 unicef – RI Future Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
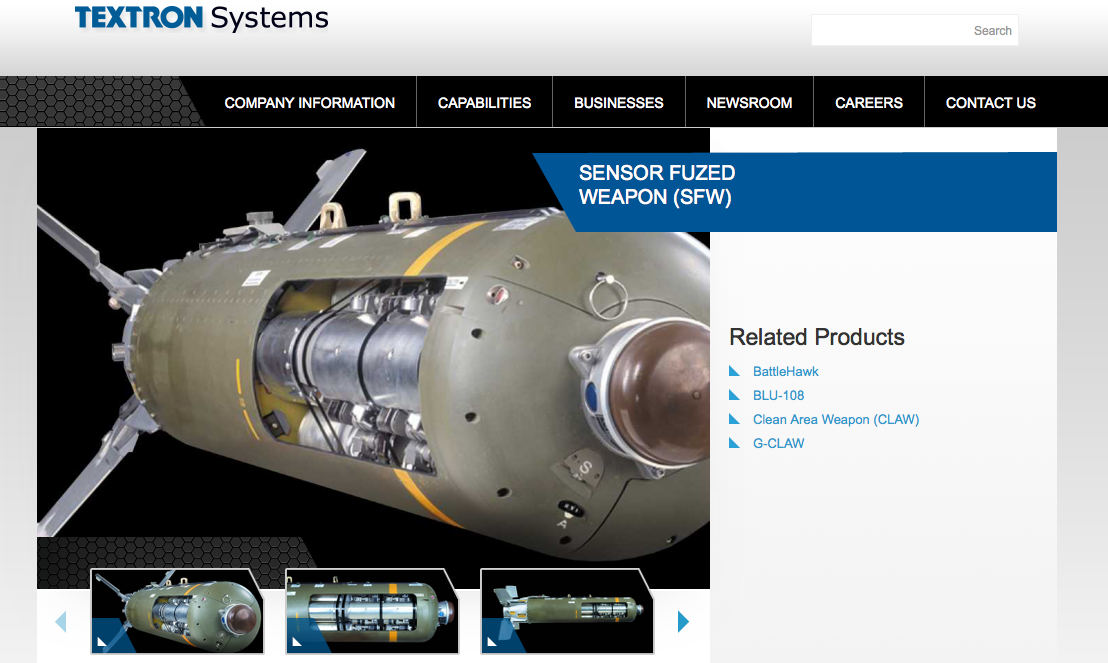
As Saudi Arabian airstrikes threaten to cause a humanitarian crisis in Yemen, the American Friends Service Committee of Southeastern New England is planning to protest Textron outside the company’s headquarters in Providence.
“We will gather at 4:30pm with the long budget banner and signs addressing the use of Textron-made cluster bombs by Saudi Arabia in Yemen and a call for our taxes to be invested in addressing human needs not militarization,” according to a notice from AFSC-SENE, a Quaker organization that advocates for peace and justice.
In February, Human Rights Watch criticized Saudi Arabia for its use of cluster munitions against Yemen. The report details civilian injuries and calls out the Textron-made bomb for malfunctioning more than 1 percent of the time – a violation of US trade policy. Last week, the World Health Organization said 6,200 people have died since the conflict began in March of last year and more than 30,000 were injured. The United Nations said this week more than 900 children have been killed since the conflict began, more than seven times more than the previous year.
Cluster bomblets & other unexploded ordnance are a particular hazard to young children. Warning poster in #yemenpic.twitter.com/tXIuX9BlsE
A New York Times report yesterday said the Saudi led airstrikes threaten to cause a “humanitarian catastrophe in Yemen, one of the world’s poorest countries” and listed cluster bombs as a contributing factor. “In addition to airstrikes, civilians must contend with hazards posed by unexploded bombs and cluster munitions dropped by the Saudi coalition.”
There are 118 nations that officially condemn the use of cluster bombs. The United States and Saudi Arabia are not among them.
The April 18 protest will include delivering letters to senators Jack Reed and Sheldon Whitehouse, both of whom expressed to RI Future a desire to better address the use of cluster bombs. Whitehouse is a co-sponsor of the Cluster Munitions Civilian Protection Act, which would add regulations to the use and sale of cluster bombs. The US already imposes some restrictions on the use and sale of cluster bombs. Textron is the only American company that makes cluster bombs, though there is at least one other company that makes a component of Textron’s cluster bomb.
“Shortly after we gather we will send someone to Senator Whitehouse’s and Senator Reed’s offices with a letter asking them to at the very least support the People’s Budget and to vote against a budget that spends war on militarism than all other things put together,” said the AFSC-SENE announcement. “We will also have a letter calling on Textron to stop the manufacture of these weapons.”
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
The author, Dr. Fatoumata Sangare, in Gandiol, Senegal.
As a medical doctor who graduated from the Faculty of Medicine of Mali, West Africa in 2001, I saw firsthand the tremendous healthcare difficulties that underserved populations, especially women and children, faced due to poor policies.
For example, during my two-year internship at Point G Hospital in Mali, the pulmonary service had two main units. One set aside for patients with non-tuberculosis diseases was never full, but the one designed for patients with tuberculosis functioned beyond its capacity, turning away many patients and redirecting them to other facilities. Despite poor working conditions, long hours, and minimal essential resources, I dedicated myself to my patients and made a personal commitment to increase the hospital’s resources, never again turning away needy patients or denying medical care.
Another experience that shaped me was when a 12-year-old boy in the final stage of pulmonary tuberculosis died in my arms the day after admission. The boy came from a remote village where health care facilities and road infrastructures for easy access to the closest health center were non-existent. This made me realize that there are too many children in Mali who don’t have access to proper health care.
These events and other experiences in various clinical settings fueled my determination to help underserved populations in my homeland and other West African countries. Since then I’ve been in the United States gaining more education in the highly specialized field of public health, particularly in infectious diseases, so that I can soon become a part of an effective health care system in West Africa.
A lot has changed in West Africa since 2001 with the enactment of the Millennium Development Goals (MDGs), a set of 8 global goals for reducing the root causes of poverty by 2015. According to World Health Organization (WHO) 2014 data, improvements have been made to the health systems in Mali and other West African countries. Mali has reduced by two-thirds the under-five mortality rate between 1990 and 2015, and maternal mortality has been reduced by three-quarters. Senegal, Benin and Nigeria have also made much progress. Niger has achieved the MDG for child survival by reducing by two-thirds the under-five mortality rate.
Despite the progress made on achieving the MDGs, challenges still remain in West Africa’s health systems. UNICEF’s Progress Report (2015): A Promise Renewed indicates that although Niger has made progress, it still remains among the ten countries with the highest under-five mortality rate with 96 deaths per 1,000 live births, or nearly 1 in 10 children dying because of a lack of basic maternal and child care. Mali, Nigeria, and Benin are in similar situations.
Sadly, the 2014 Ebola outbreak further weakened the health systems in other West African nations, putting the healthcare of women and children at significant risk. Due to fear of being infected at health facilities, women stopped going to clinics for non-Ebola-related services such as family planning, pre- and post-natal services. The number of women giving birth in hospitals and health clinics dropped by 30%, according to a report by the United Development Group.
Save the Children’s 2015 report, A Wake-Up Call: Lessons from Ebola for the World’s Health Systems, reveals that 97% of children in the Monrovia suburb of Clara Town had routine vaccinations before the outbreak, yet during the outbreak only 27% were getting vaccinated. In Sierra Leone, coverage of the measles vaccine has fallen by 20% across the country in a year. Three epicenter countries suffered three to four times more cases of measles in the year of the Ebola outbreak than in the previous year. Children have been left untreated for preventable diseases. For instance, there was a 40% fall in the number of children under five treated for malaria between May and September 2015 in Sierra Leone. Moreover, travel restrictions and low agriculture productivity during the outbreak led to food shortages. As a result, children under the age of five were at serious risk of acute malnutrition in the three countries. Children also lost school hours, which makes them more vulnerable to poverty and diseases.
More recently, I experienced another personal tragedy. One of my closest friends died from postpartum hemorrhage in hospital, in Bamako, the capital of Mali, after a cesarean section. The baby did not survive either. Postpartum hemorrhage is the leading cause of maternal deaths in Mali. In addition to a lack of continuing medical education of specialized health care workers in urban settings, a large proportion of births occur at home and deliveries are carried out by unskilled birth attendants in rural areas. Furthermore, the proportion of births attended by skilled providers in health facilities remains low. The overall antenatal care coverage in the country is also insufficient.
Through my personal experiences and study of healthcare systems, I am constantly reminded that public health challenges are still ahead of us, and we still have a long path to walk to reach the unreached in West African cities and rural areas, especially women and children. No child should die from preventable diseases, and no woman should die from giving birth in the 21st century. We need to act.
The good news is that efforts are underway to help us become the greatest generation on accessing health care. The bipartisan Reach Every Mother and Child Act of 2015 was recently introduced by Senator Collins and Coons and Representatives Reichert, McCollum, Lee and McCaul (S. 1911 and H.R. 3706). The bill lays out a road map for ending preventable maternal and child deaths by 2035 largely by reforming current efforts to enact smarter and more effective approaches to saving more lives. Returns will be measured in lives saved and healthy prosperous communities.
The Reach Act enshrines into law the need for:
An ambitious, coordinated U.S Government strategy with clear, measurable goals and increasing accountability and transparency at all levels for ending preventable maternal and child deaths and helping ensure healthy lives by 2035.
Focusing on the poorest and most vulnerable populations in 24 partner countries; and recognizing the unique needs within different countries and communities.
Scaling up the most evidence-based interventions with a focus on country ownership by requiring a coherent all-of- government plan on maternal and child health.
Enshrining a Child and Maternal Survival Coordinator responsible for oversight and coordination of resources directly linked to reducing maternal and child mortality.
Creating new innovative funding sources to complement U.S. investments.
Senators Reed and Whitehouse, and Representatives Langevin and Cicilline have expressed support, but have not yet cosponsored the bill – they should cosponsor in the increase the likelihood that these important reforms are enshrined into law. In passing the legislation, they will enhance US leadership on serving underserved populations, especially women and children; furthermore, this strategy that puts kids and mothers first give us the chance to make sure every child regardless of where he/she’s born has healthy start to life. The bill does not call for additional dollars, only that we make the best possible use of the dollars we do spend. As I discovered in my work in Mali, policies can make all the difference in the world.
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387
Deprecated: Function get_magic_quotes_gpc() is deprecated in /hermes/bosnacweb08/bosnacweb08bf/b1577/ipg.rifuturecom/RIFutureNew/wp-includes/formatting.php on line 4387

 As Saudi Arabian airstrikes threaten to cause a humanitarian crisis in Yemen, the American Friends Service Committee of Southeastern New England is planning to protest Textron outside the company’s headquarters in Providence.
As Saudi Arabian airstrikes threaten to cause a humanitarian crisis in Yemen, the American Friends Service Committee of Southeastern New England is planning to protest Textron outside the company’s headquarters in Providence.
