Over the past two weeks, this series has laid out a case for why Rhode Island is in the business of empowering veterans and what the future of state-level veterans affairs can be. But a discussion about veterans can’t occur in a media vacuum and it’s impossible to ignore sizzling headlines about the VA and presidential candidates.
Snapshot: Hillary Clinton was asked about the systemic problems at the VA recently, her response included a comment that the issues weren’t “as widespread as it has been made out to be,” and veterans (as well as congressional leaders) have taken her to task for it.
The upside is renewed media attention to a significant moral issue of our time: setting the standard for providing the highest quality and timely healthcare possible to our veterans. The continued problems with access to care are heart wrenching. Just a few months ago, I was meeting with disabled veterans who were receiving sporadic care at a VA in Texas – it was difficult to hear that they were having such a hard time after being discharged, especially when most of them received consistent and quality treatment while still in uniform.
- Part 1: After 125 years, RI veterans will finally get a director
- Part 2: Next generation Veterans’ Affairs: Economic engine, not resource hub
The truth is that, even though there are many veterans getting excellent treatment at the VA, things are still a mess. And I hope journalists continue to draw attention to the problems as well as the progress – let’s see a real-time report card of how the VA is shaping up and (finger’s crossed) celebrate the positive changes being implemented.
But the end of this series is about Rhode Island’s Veterans Affairs. The Division needs to go through it’s own metamorphosis and today, we’ll explore two seldom discussed obstacles it will need to tackle to get there.
ONE: Inter-Generational Collaboration
About half of the 72,000+ veterans in the state of Rhode Island are over the age of 65. Who are these vets? Check out the infograph:

While some veterans who served in Vietnam are a bit younger, many are 65 or older. And when talking about veterans, the era you served in matters. The obvious difference is how these veterans were received during their transition home; the starkest contrasts are between WWII, Vietnam, and Post-9/11 Vets. WWII veterans came home to parades while Vietnam veterans were faced with protests. Post-9/11 veterans are received with some fanfare, along with Yellow Ribbon bumper stickers and interesting “thank you” hand gestures. These differences have had a lasting impact on how these veterans see themselves and other-era vets.
Another huge difference is the level of participation in traditional veterans’ organizations. Older veterans comprise the majority of organizations like the VFW and American Legion – important groups that have been struggling to attract younger veterans (there are exceptions). This highlights the evolving way that veterans connect and what they view as useful as they come home.
Bottom Line: The Division will have to invest time and energy into developing not only a robust digital media platform, but strengthening inter-generational relationships with engaging, purpose driven programs.
TWO: Redefining the Veteran Identity

The first time I came home to Bristol, I wrestled with the title, “veteran.” While doing outreach in Boston, I learned I wasn’t alone. All veterans coming home have to answer the question: Who am I now? There are roughly three answers:
- I’m a veteran living amongst civilians.
- I’m a veteran and a civilian.
- I’m a civilian – forget about the veteran stuff.
Understanding what informs these different ways vets identify is crucially important to not only their successful transition but also creating a strong, vibrant veteran community in our state. The less someone identifies as a veteran, the harder it is to find them. And you have to identify and engage veterans before you can empower them. Ask any Veterans Service Officer or student veteran who’s attempting to organize – they’ll tell you that attracting veterans en masse is difficult. But here’s a shout out to a few organizations I think are getting it right and broadening the veteran identity: Team Rubicon, The Mission Continues, and The 6th Branch.
Bottom Line: The Division will have to rally around an outreach message that resonates with folks who don’t necessarily think of themselves as veterans first but who would jump at the chance to serve a greater good.
The challenges we see at the federal level are daunting. But in Rhode Island, there are plenty of readily accessible opportunities to improve the lives of veterans and our community. From accelerating the transition process for new veterans to completely reshaping the way we do outreach, the next decade has the potential to be an exciting time to be a veteran in Rhode Island. The biggest risk our state takes is in not seizing this moment. My challenge to our leaders this Fall: shake things up and make some waves.
This is the last of a 3-part series covering veterans affairs in Rhode Island: Part One | Part Two
Want to be the new Director of the Division of Veterans Affairs? Apply by November 6th!























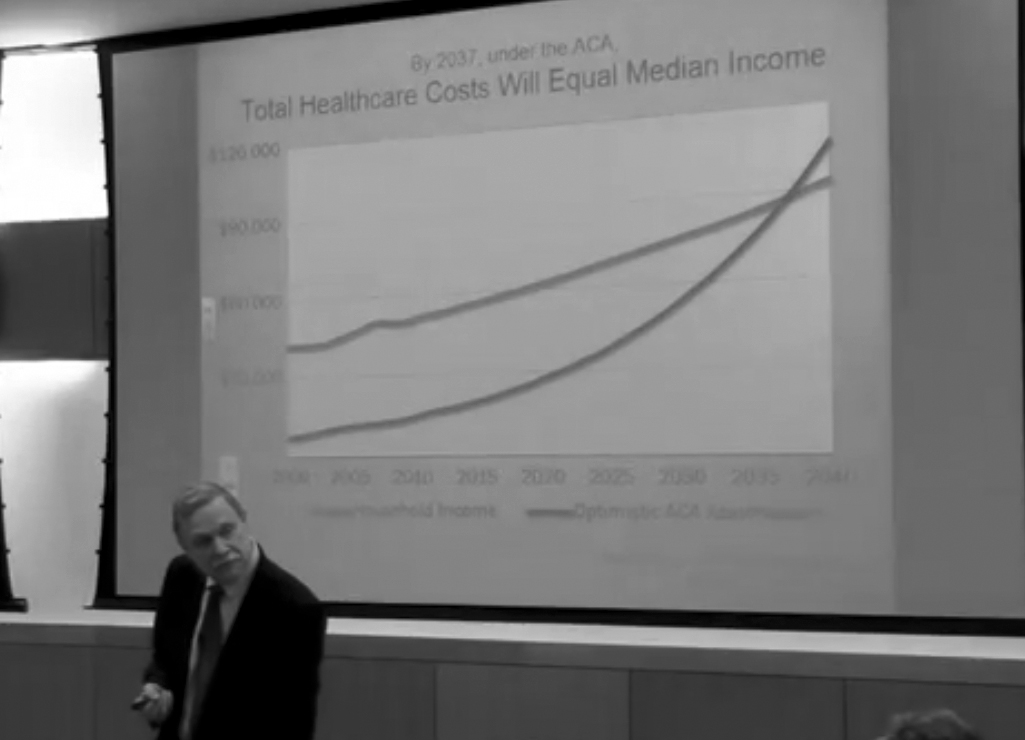
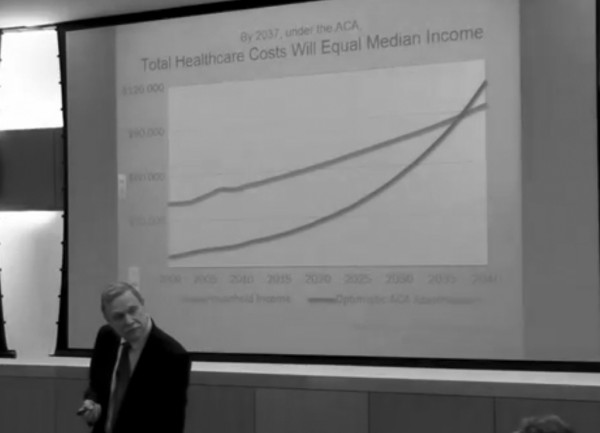
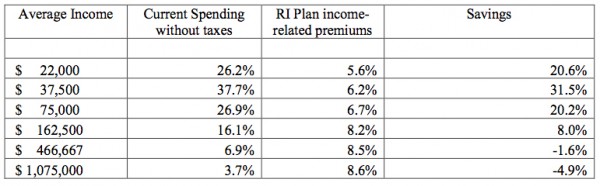 Representative Aaron Regunberg, from the East Side’s District 4, is planning to introduce legislation for a statewide single payer healthcare plan this session. Model legislation from the PNHP is available
Representative Aaron Regunberg, from the East Side’s District 4, is planning to introduce legislation for a statewide single payer healthcare plan this session. Model legislation from the PNHP is available 






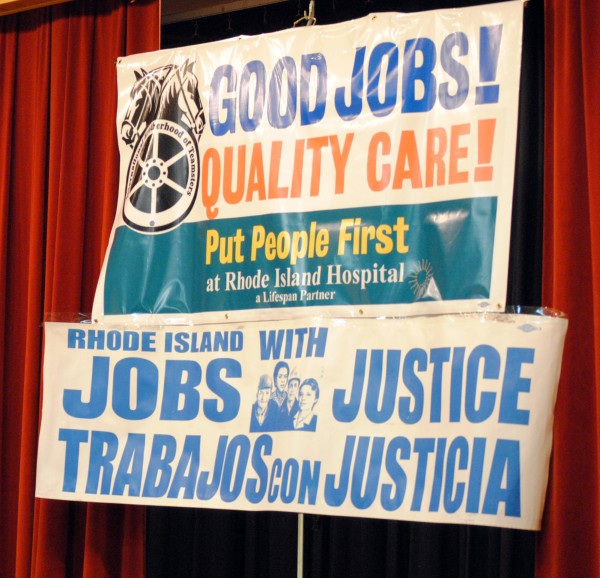
 More than 500 people crowded into the meeting room of Our Lady of the Rosary Church on Benefit St in Providence for the
More than 500 people crowded into the meeting room of Our Lady of the Rosary Church on Benefit St in Providence for the  According to Local 251, “As a non-profit entity, Lifespan and RI Hospital are supposed to put the healthcare needs of the community first. Unfortunately, management has taken cost cutting measures, causing shortages in equipment and staff that undermine patient care.”
According to Local 251, “As a non-profit entity, Lifespan and RI Hospital are supposed to put the healthcare needs of the community first. Unfortunately, management has taken cost cutting measures, causing shortages in equipment and staff that undermine patient care.” Obamacare has allowed Lifespan/RI Hospital to take in an additional
Obamacare has allowed Lifespan/RI Hospital to take in an additional  The Speakout was intended to show community support for the workers of RI Hospital, and was attended by Representatives David Cicilline and Jim Langevin, as well as General treasurer Seth Magaziner. There were also representatives from many other unions and community groups such as Jobs with Justice, Unite Here! and Fuerza Laboral. Many religious leaders, including Father Joseph Escobar and Rev Duane Clinker, were on hand to show support.
The Speakout was intended to show community support for the workers of RI Hospital, and was attended by Representatives David Cicilline and Jim Langevin, as well as General treasurer Seth Magaziner. There were also representatives from many other unions and community groups such as Jobs with Justice, Unite Here! and Fuerza Laboral. Many religious leaders, including Father Joseph Escobar and Rev Duane Clinker, were on hand to show support.